The decrease in death from abdominal aortic aneurysms in recent decades may not be due to increased screening. In fact, University of Gothenburg scientists argue that increased screening may be putting patients in unnecessary danger. In their new study, they show how the recommendations for who should and who should not be screened might need to be revised.
Abdominal aortic aneurysms, detectable via a general ultrasound scan, are becoming less common, but regular screening continues. "You run the risk of both over-diagnosing and over-treating a disease that does not at all represent the same problem anymore, which is a very positive development," explained lead author Minna Johansson.
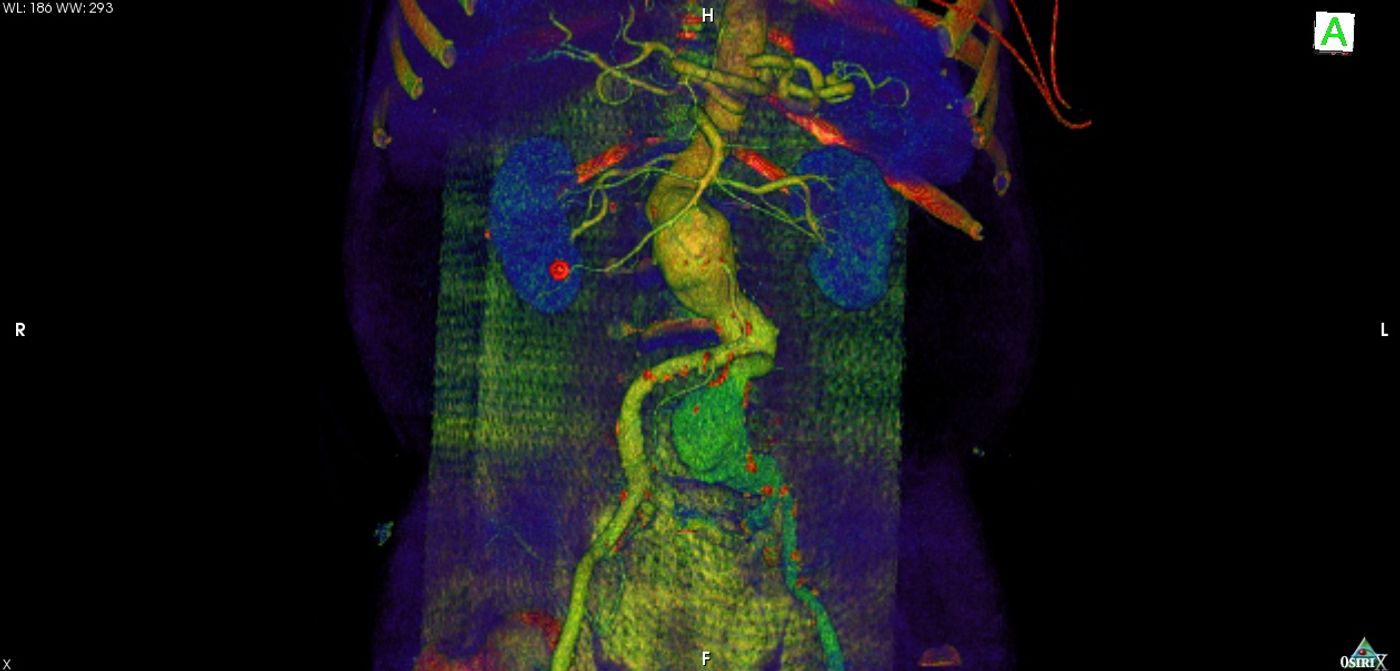
Approximately 200,000 people are diagnosed with an abdominal aortic aneurysm every year, with a large proportion being men older than 55. This type of aneurysm occurs when the abdominal aorta, which supplies blood to the legs, enlarges as the blood vessel walls weaken. Risk of an abdominal aortic aneurysm is much higher in regular smokers, and the risk is also increased risk if a first-degree family member also has or had an abdominal aortic aneurysm.
There are usually no symptoms of an abdominal aortic aneurysm. That is, until it ruptures – where there is less than a 20 percent chance that the affected person will live. Thus, regular screening protocols were enacted with the goal of detecting aneurysms and conducting preventative surgery to prevent rupture.
The problem with this screening approach is that some aortic aneurysms identified by regular screening would never have caused any problems. But when this type of aneurysm is identified, preventative surgery is still done. And with any surgery, especially in older people, risks of complications and death accompany the procedure.
University of Gothenburg scientists conducted their study by comparing 24,265 older men who were screened for aneurysms with 106,087 men who were not screened. They also analyzed the incidence of and mortality from abdominal aortic aneurysms between 1987 and 2015. Mortality declined in both screened and unscreened populations.
"If the screening program had any impact at all on the decline, it was very small,” Johansson said. “This very positive reduction in mortality was probably due to a decline in smoking.”
However, the medical community seemed to believe that the decrease in mortality was thought to be because of increased screening, so doctors continued to do regular screening. Johansson says that this increases the risk of over-diagnosis and over-treatment. And while a handful of men out of thousands over several years might be saved from a ruptured abdominal aortic aneurysm, many more will be diagnosed when treatment isn’t necessary, and some will receive surgery when there’s no benefit but all the risk.
Johansson offers an alternative solution: screening for only high-risk men - current and former heavy smokers and those with a family connection to an aortic aneurysm.
"This is a difficult ethical dilemma. It's important that the men who are summoned for screening are informed that there are serious risks arising from participation and that the chance to benefit is at best very small today,” Johansson concluded. “We came to the conclusion that it is doubtful that the benefits of screening outweigh the harms and that the Swedish screening program should therefore be revisited.”
The present study was published in the journal The Lancet.
Sources: Society for Vascular Surgery, University of Gothenburg