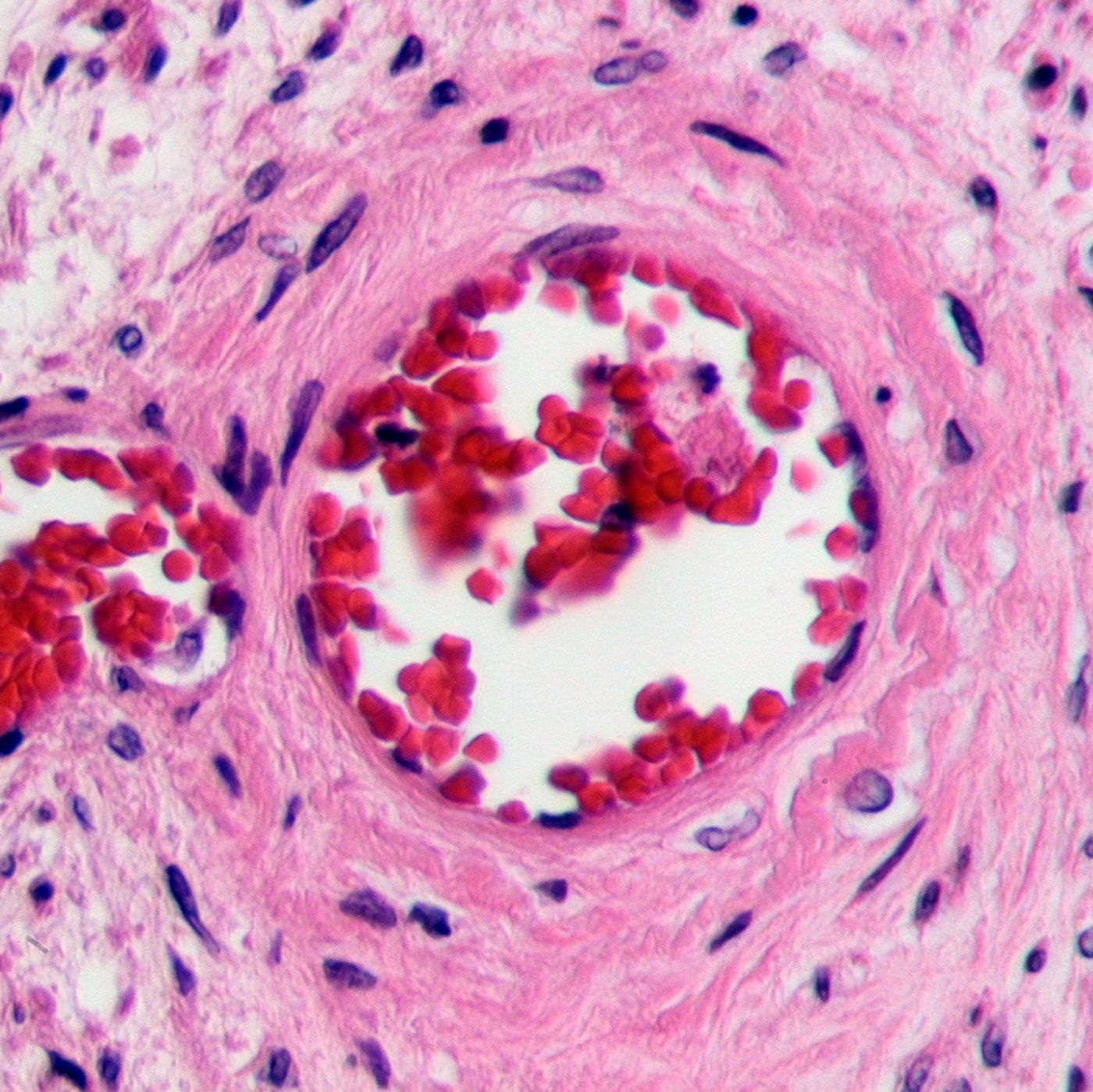
Rare but deadly, thrombotic thrombocytopenic purpura (TTP) is a disease where blood clots block the smallest blood vessels often leading to kidney failure, stroke, and heart disease. Over 4 million Americans are affected each year, either from hereditary or acquired forms of the disease.
Past the acute phase, TTP is relatively easily defeated with immunotherapy, said Paul Knöbl from the Medical University of Vienna. However, 10 to 20 percent of people do not survive the acute phase, even with plasma exchange therapy. In a new study published in the
New England Journal of Medicine, Knöbl and other researchers from the Medical University of Vienna examined the capability of a synthesized antibody to reverse the impact of the disease.
TTP is characterized by a deficiency of an enzyme called ADAMST13 regardless of whether the disease was acquired or inherited. Without ADAMST13, another protein called von Willebrand is overexpressed and destructively so, binding platelets and inducing aggregation in blood vessels. Blood clots caused by TTP can lead to kidney failure, stroke, and heart disease.
Current plasma exchange therapy removes autoantibodies causing the ADAMST13 deficiency, removes overgrown von Willebrand protein complexes, and replenishes the body’s stock of ADAMST13. After a patient survives the acute phase, immunotherapy prevents continuous autoantibody formation. The synthesized antibody proposed by this study would be used for treatment both during and after the acute phase, instead targeting the masses of overactive von Willebrand protein. By blocking the protein’s interaction with platelets, the antibody reduces the severity of blood clots characterizing TTP to practically zero.
"In future this drug might also be used to treat similar diseases, which are jointly caused by overactivity of the von Willebrand factor, and therefore represents a new treatment option," said the Medical University of Vienna’s Bernd Jilma.
The antibody being studied is called “caplacizumab.”
Source:
Medical University of Vienna,
New England Journal of Medicine