The immune system must be able to swing into action to overcome pathogenic invaders. But the inflammation that accompanies the immune response must be carefully controlled, or it can lead to serious, sometimes critical medical problems. Since the onset of the COVID-19 pandemic, researchers and clinicians have noticed that in some people, the viral infection leads to excessive inflammation. Reporting in Nature, scientists found an explanation for the severe inflammation that can be caused by COVID-19, which can damage organs. This research also found that antibodies that are produced after a COVID-19 infection, but not mRNA vaccination, sometimes trigger more inflammation.
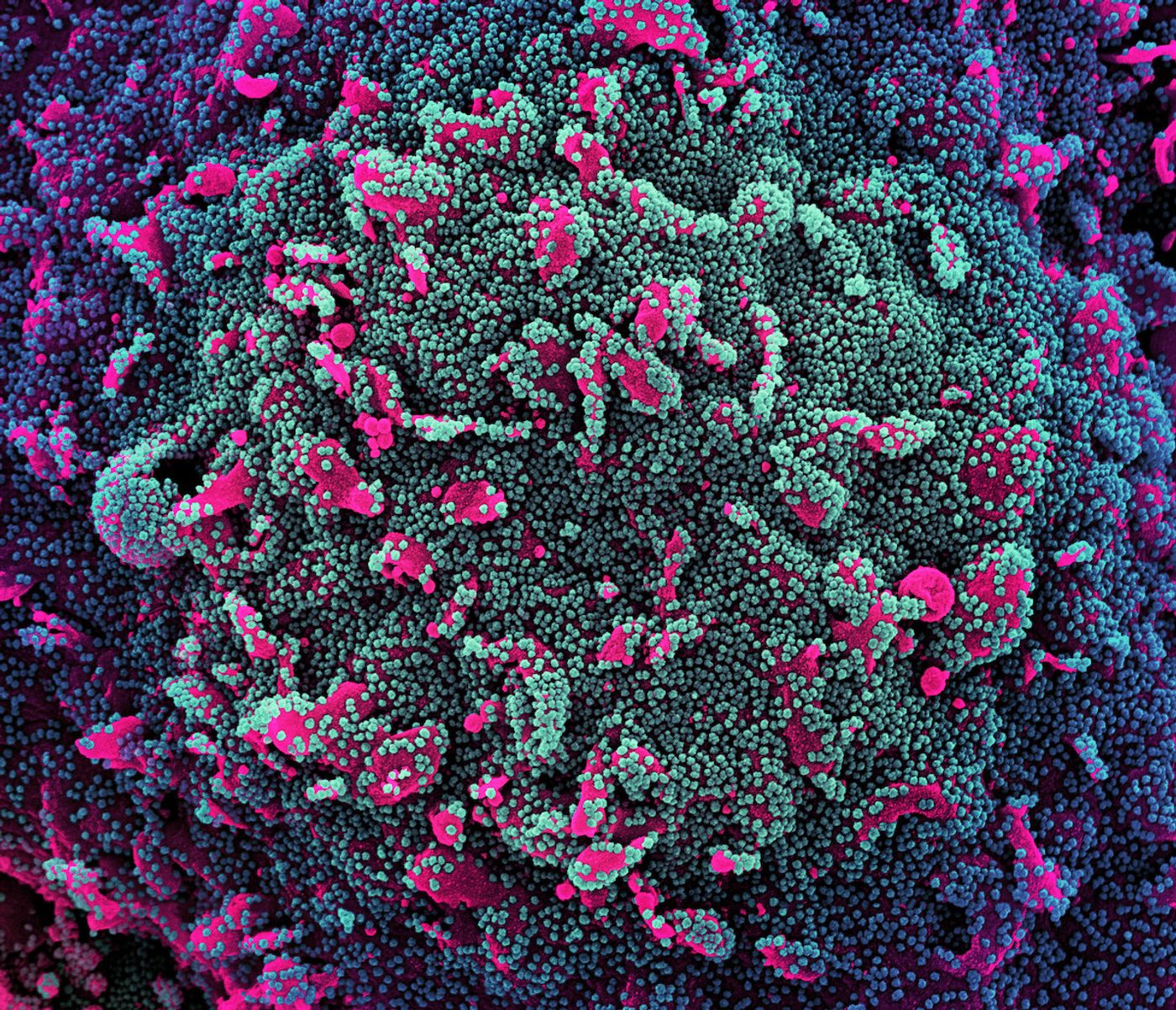
Colorized scanning electron micrograph of a cell (pink) heavily infected with SARS-CoV-2 virus particles (teal and purple), isolated from a patient sample. Image captured at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland. Credit: NIAID
In this study, the researchers set out to find how patients with a mild versus severe COVID-19 differed, explained study co-leader Judy Lieberman, MD, Ph.D. of Boston Children's Hospital. The scientists assessed blood samples from COVID-19 patients admitted to the Massachusetts General Hospital emergency room, and compared them to samples from healthy people as well as respiratory disease patients.
This work revealed that the SARS-CoV-2 virus, which causes COVID-19, infects two types of immune cells called monocytes and macrophages. About ten percent of monocytes and eight percent of macrophages in the lungs of infected patients were found to be infected. Both cells undergo a process called pyroptosis when they die, which unleashes powerful inflammatory signals on the immune system.
"In the infected patients, about six percent of blood monocytes were dying an inflammatory death," said Lieberman. "That's a large number to find, because dying cells are rapidly eliminated from the body."
Post-mortem lung tissue from individuals that died of COVID-19 was also analyzed in this study. This indicated that about a quarter of the macrophages in that tissue had died.
The SARS-CoV-2 virus is known to use a receptor called ACE2 to enter cells, and monocyte and macrophages have low levels of that receptor, making these findings a surprise. While the virus infects these cells, it doesn't seem to replicate there. The researchers suggested that can't happen because the immune cells die too quickly for the virus to start replicating. While that has a protective effect, noted Lieberman, it also causes the release of inflammatory molecules that can be harmful. "In people who are more prone to inflammation, such as the elderly, this can get out of control."
This study also found that monocytes that carry a receptor called CD16 are more likely to be infected. This type of monocyte is not common, but the study indicated that there are unusually high numbers of these cells in COVID-19 patients. The CD16 receptor seems to recognize antibodies that bind to the SARS-CoV-2 spike protein, but such antibodies may actually help the virus infect cells. "The antibodies coat the virus, and cells with the CD16 receptor then take the virus up," Lieberman explained.
Patients that had received a COVID-19 vaccine did not carry antibodies that enhanced infection, however. The researchers suggested that the vaccine-generated antibodies may not bind to CD16 efficiently, eliminating the infection-enhancing effect.
The study may also explain why monoclonal antibodies are only helpful in the earliest stages of infection. The treatment could be promoting inflammation if given later, suggested Lieberman, but more research will be needed to confirm that hypothesis. "We may need to look at the properties of the antibodies," added Lieberman.
Experienced research scientist and technical expert with authorships on over 30 peer-reviewed publications, traveler to over 70 countries, published photographer and internationally-exhibited painter, volunteer trained in disaster-response, CPR and DV counseling.