

Cardiology
Meditation Helps Smokers Quit
I currently work at a small CRO involved in clinical trial management.
Pain. The meaning of sense of pain has been debated for decades, even centuries. Saint Augustine once remarked, "The greatest evil is physical pain”. But what is pain? Pain has both physical and subjective properties, but doctors and clinicians have come to rely only on subjective reports of pain. The problem with this is that people vary in how painful they perceive their pain to be. This can be a difficult measure to use for a diagnosis. However, researchers from the Indiana University School of Medicine recently published in Molecular Psychiatry a paper detailing their findings of an objective biomarker that can be measured to determine the level of pain.
Photo source: pexels.com
Neurologically speaking, there are chemical messengers, nervous system pathways, and brain regions all involved in sending a signal to the brain that the body has been damaged in some way. Let us imagine a needle prick on the finger. Ouch! This immediately releases chemical messengers, such as histamine, bradykinin, and prostaglandins. These chemical messengers are recognized by specialized neuron cell types whose receptors are in the cutaneous tissue of our skin.
These specialized neurons send their signals to the spinal cord, and then things get a little complex. Pain is "sensed" via a number of complex signal mechanisms that send the message up to the brain. Interestingly, the pain can also be mediated by down-stream signals from the brain, which helps modulate the "subjective" nature of the pain. The subjective nature of pain depends on situational and/or emotional factors. Panic and fear can decrease the sense of pain (get out of this situation fast, we'll feel the pain later!), while depression or chronic stress can increase it (I'm so stressed out, ow I just stubbed my toe, it hurts so much, I can't handle it!).
Photo source: PixaBay.com
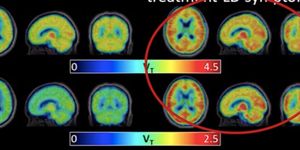
Thus, you can see the complicated nature involved in sensing and perceiving pain. How the researchers were able to find a biomarker for this process is truly remarkable. Scientist Dr. Alexander Niculescu and colleagues took advantage of the fact that, as mentioned above, certain mental states can manipulate the patient's experience of pain. They relied on a population of approximately 400 psychiatric patient participants. Their reasoning was that, according to the paper, "Psychiatric patients may have an increased perception of pain, as well as increased physical health reasons for pain, due to their often adverse life trajectory".
The researchers were able to find a handful of genes that correlated to pain state and of future emergency department (ED) visits for pain. The genes which the scientists were able to correlate with pain were MFAP3, GNG7, CNTN1, LY9, CCDC144B, and GBP1. Using bioinformatic drug repurposing analyses, they were able to find novel drug compounds that would selectively target these genes and could be used to not only measure pain level but also inform the drug discovery process to use these genetic biomarkers to create more personalized treatments for pain.
Below is a video going into a bit more detail about how we perceive pain.
Video source: YouTube.com
Sources: The Soliloquies of St. Augustine, Molecular Psychiatry, AACN Clinical Issues, Clinical Care, Advances in Wound Care